

“Different clinical and pathological features characterise the diverse clinical pulmonary hypertension (PH) groups”1 The following, most up-to-date version of the classification is as follows:
1 PAH
1.1 Idiopathic PAH
1.2 Heritable PAH
1.3 Drug- and toxin-induced PAH
1.4 PAH associated with:
1.4.1 Connective tissue disease
1.4.2 HIV infection
1.4.3 Portal hypertension
1.4.4 Congenital heart disease
1.4.5 Schistosomiasis
1.5 PAH long-term responders to calcium channel blockers
1.6 PAH with overt features of venous/capillaries (PVOD/PCH) involvement
1.7 Persistent PH of the newborn syndrome
2. PH due to left heart disease
2.1 PH due to heart failure with preserved LVEF
2.2 PH due to heart failure with reduced LVEF
2.3 Valvular heart disease
2.4 Congenital/acquired cardiovascular conditions leading to post-capillary PH
3. PH due to lung diseases and/or hypoxia
3.1 Obstructive lung disease
3.2 Restrictive lung disease
3.3 Other lung disease with mixed restrictive/obstructive pattern
3.4 Hypoxia without lung disease
3.5 Developmental lung disorders
4. PH due to pulmonary artery obstructions
4.1 Chronic thromboembolic PH
4.2 Other pulmonary artery obstructions
5. PH with unclear and/or multifactorial mechanisms
5.1 Haematological disorders
5.2 Systemic and metabolic disorders
5.3 Others
5.4 Complex congenital heart disease
PAH: pulmonary arterial hypertension; PVOD: pulmonary veno-occlusive disease; PCH: pulmonary capillary
haemangiomatosis; LVEF: left ventricular ejection fraction.
The World Symposium on Pulmonary Hypertension in 2018 updated the classification outlined in the 2015 ESC/ERS clinical guidelines on the diagnosis and treatment of pulmonary hypertension1 to draw attention to PAH long term responders to calcium channel blockers. Sections 1’ and 1’’ were renumbered within the group of PAH. Classification updates were also made in groups 2, 3 and 4.
What is the WHO functional class?

The World Health Organization (WHO) functional class describes how severe a patient’s pulmonary hypertension (PH) symptoms are.2 There are four different classes – I is the mildest and IV the most severe form of PH. Assigning a functional class helps the PH healthcare team to understand how the patient is affected by their condition. A goal of PH treatment is to make everyday living easier, so it is very important to have an accurate picture of how PH is affecting a patient’s daily life.
How are patients assigned to a WHO functional class?
To assign a patient to a WHO functional class, the PH healthcare team will ask questions to find out how PH is affecting them.
What is the risk assessment under ESC/ERS guidelines?
In order, however, to describe the severity of the disease, the risk assessment, including various measures as described in the ESC/ERS guidelines, is to be conducted.
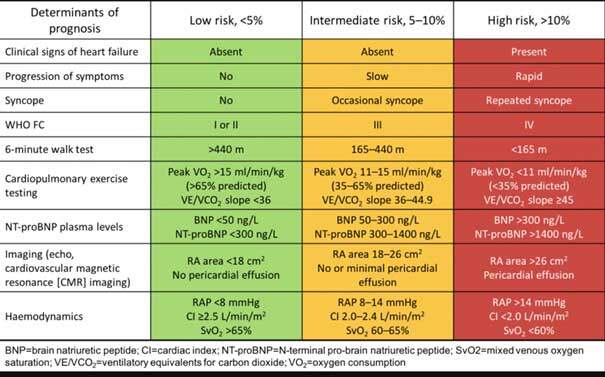
Source: ESC/ERS guidelines
Why is it important for patients to keep track of their PH symptoms?
The main aim of PH treatment is to improve a patient’s symptoms – ideally to WHO functional class I or II.3 It is helpful for patients to take note of how they are feeling, and write down if they have found something easier or more difficult. This record of symptoms gives the healthcare team more information about how their patient has been getting on since the last clinic visit, and helps them to make decisions about their future treatment.
Reviewed by Prof. Simon J Gibbs
Last medical update: 05/30/2020
Sources
- ESC/ERS guidelines https://www.escardio.org/static_file/Escardio/Guidelines/Publications/PAH/2015%20ESC-ERS%20Gles%20PH-Web%20addenda-ehv317.pdf
- McGoon M, Gutterman D, Steen V et al. Screening, early detection, and diagnosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004;126(1 Suppl):14S–34S.
- Galiè N, Hoeper MM, Humbert M et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 2009;30:2493–537.